
By Dr. Gavin McAuley | EMPOWERVIDA
THE SHORT ANSWER
Yes — they are metabolic partners. B12 and folate work together in the methylation cycle, one of the most important biochemical pathways in your body. Supplementing one without the other can mask a dangerous deficiency of the other. They should always be considered as a pair.
Why They Are Inseparable
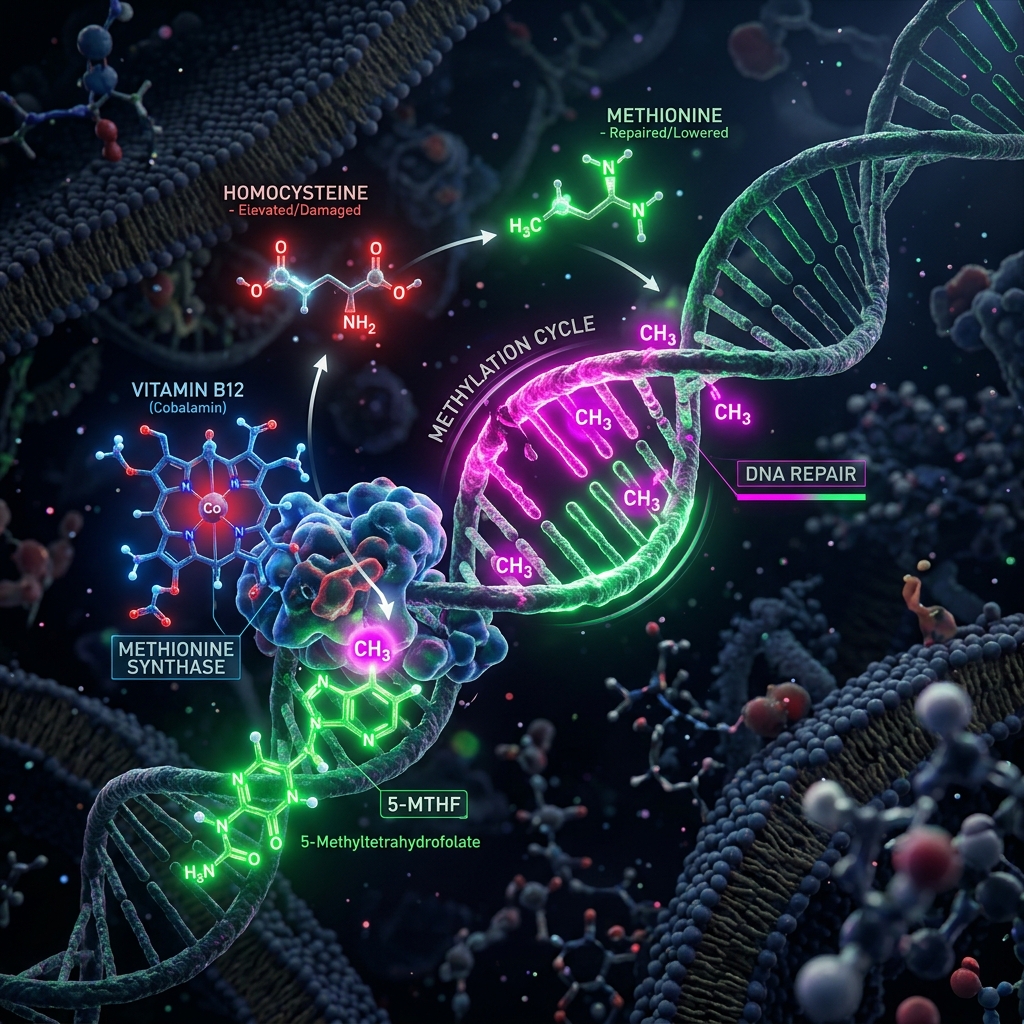
B12 and folate are co-dependent enzymes in the methylation cycle — the biochemical process your body uses to make DNA, regulate gene expression, produce neurotransmitters (serotonin, dopamine, melatonin), and detoxify homocysteine. Without adequate B12, folate becomes trapped in an unusable form (methyltetrahydrofolate trap). Without adequate folate, B12 cannot complete its role in homocysteine metabolism.
The clinical consequence: elevated homocysteine. This amino acid is an independent risk factor for cardiovascular disease, stroke, and cognitive decline. Both B12 and folate are required to convert homocysteine back into methionine (a safe, useful amino acid). When either is deficient, homocysteine accumulates and damages endothelial cells lining your blood vessels.
The Masking Danger
Here is the critical safety issue: high-dose folate can mask B12 deficiency. Both vitamins are required that allows red blood cells to mature properly. In B12 deficiency, you develop megaloblastic anaemia (large, immature red blood cells). But if you supplement folate alone, it can partially correct the anaemia — making blood tests appear normal — while the neurological damage from B12 deficiency continues silently. This is why folic acid fortification of foods remains controversial in some medical circles.
The neurological damage from untreated B12 deficiency includes peripheral neuropathy (tingling, numbness in hands and feet), cognitive impairment, and irreversible subacute combined degeneration of the spinal cord. By masking the blood picture, isolated folate supplementation can delay B12 diagnosis by months or years — long enough for permanent nerve damage to occur.
Dosing and Forms
B12: 1,000mcg daily as methylcobalamin (the active, methylated form). Cyanocobalamin is the synthetic form — it requires conversion and some people (those with MTHFR polymorphisms) convert it poorly. Sublingual tablets bypass potential gut absorption issues.
Folate: 400-800mcg daily as methylfolate (5-MTHF) rather than synthetic folic acid. Approximately 30-40% of the population carries an MTHFR gene variant that impairs conversion of folic acid to its active form. Methylfolate bypasses this entirely.
Timing: Morning, with or without food. Both are water-soluble and well-absorbed at any time. Many people find B-vitamins mildly energising, so morning dosing avoids potential sleep interference.
Who Needs This Most
Vegans and vegetarians: B12 is found exclusively in animal products. Supplementation is not optional — it is essential.
Adults over 50: Gastric acid production declines with age, reducing B12 absorption from food by up to 30%.
Patients on metformin: This common diabetes medication depletes B12 over time. If you take metformin, ask your doctor to check B12 annually.
Patients on PPIs: Proton pump inhibitors reduce stomach acid needed for B12 liberation from food proteins.
Anyone with elevated homocysteine: The B12+folate combination is the first-line treatment.
An Educational Perspective: I check homocysteine levels on virtually every patient. It is an inexpensive, under-ordered test that reveals methylation status at a glance. When homocysteine is above 10 micromol/L, the combination of methylcobalamin (1,000mcg) and methylfolate (800mcg) typically normalises it within 8 weeks. Observations have shown fatigue, brain fog, and even mood disorders improve dramatically once methylation is optimised. This is one of the highest-yield, lowest-risk interventions in functional medicine.
Explore the Pillar Topic
This article belongs to our core medical pillar on The Physician's Protocol Overview. For a comprehensive, physician-guided deep dive into this topic, read the full foundational guide.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. If you suspect B12 deficiency or have neurological symptoms, seek medical evaluation promptly.