
By Dr. Gavin McAuley | EMPOWERVIDA
TL;DR
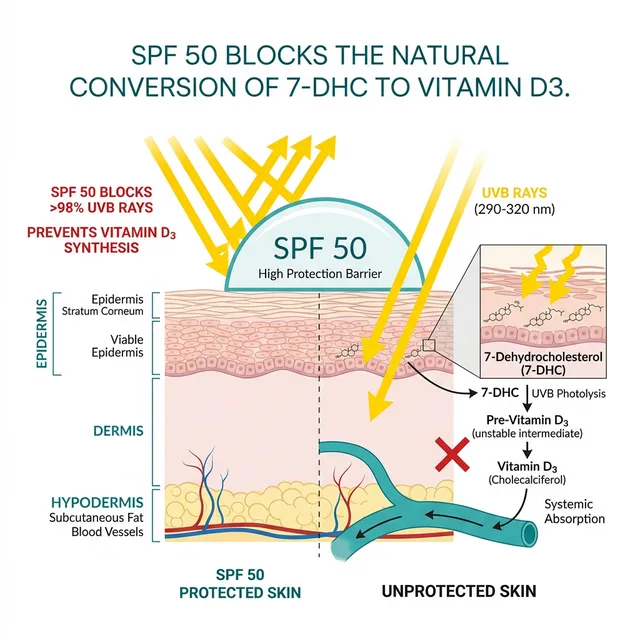
Vitamin D is not just a vitamin for bone health; it is a master neuro-steroid that governs our immune system and mood. In our modern quest to avoid skin cancer, aggressive use of SPF 50 blocks 98% of the UVB rays required to synthesise Vitamin D. The consequence? A silent, global epidemic of Vitamin D deficiency that manifests as chronic winter fatigue, compromised immunity, and depression. Discover the "Architect's Protocol" for achieving adequate D3 levels without compromising your skin health.
The Physician’s Perspective: The "Normal" Patient
In clinical practice, patients frequently present with complaints of overwhelming fatigue, severe afternoon "brain fog," and a pervasive lethargy they often mistake for clinical depression. Many are already considering or requesting SSRI medications.
However, when full blood panels are conducted, the underlying pathology often reveals profound Vitamin D deficiency—frequently dipping as low as 14 ng/mL (optimal is 50-80 ng/mL). These patients are not necessarily depressed in the traditional psychiatric sense; they are biologically starved of a critical neuro-steroid.
She was a victim of the modern "Sun Phobia." We apply SPF 50 every day, work indoors from 9 to 5, and then wonder why our biology collapses.
This case is not unusual. It is the norm. Reading Dr. Michael Holick's landmark 2007 paper in the New England Journal of Medicine was one of the biggest turning points in my medical career. It showed me how profoundly conventional medicine had undervalued this molecule — treating it as just a bone nutrient when in reality it is a master regulator of immunity, mood, and cellular function. Since then, I have persuaded patients and family members to take Vitamin D consistently, and the improvement in vitality is not subtle. It is noticeable. People come back and tell me they feel like a different person.
Here is the problem: the standard laboratory "normal" range for Vitamin D is 30-100 ng/mL. So An individual with a level of 32 gets told they are "normal." But in functional environments, we do not settle for normal. A Vitamin D of 32 is the bare minimum to prevent rickets — it is nowhere near the level required for optimal immune function, mood regulation, and neuroprotection. Functional approaches often aim for 60-80 ng/mL in every patient. The difference between a Vitamin D of 32 and a Vitamin D of 70 is the difference between surviving and thriving. Yet most GPs never mention this because, technically, both are "within range."
The Misunderstood Neuro-Steroid
Calling it "Vitamin" D is actually a historical mistake. It is not a vitamin (a compound you must get from food). It is a highly potent secosteroid hormone.
We naturally synthesise this hormone in our skin when a cholesterol derivative (7-DHC) is exposed to ultraviolet B (UVB) radiation from the sun. The liver and kidneys then convert it into its final, active form (Calcitriol), where it acts as a molecular "skeleton key."
Active Vitamin D unlocks over 1,000 different genes in the human genome. And crucially, many of those genes are located directly in the brain.

We have discovered dense clusters of Vitamin D Receptors (VDRs) in the hypothalamus, the hippocampus, and the substantia nigra. These are the exact brain regions responsible for regulating our mood, sleep-wake cycles, and dopamine production.
When you aggressive block UVB rays with daily SPF, you shut down the production of the very neuro-steroid your brain needs to maintain its emotional equilibrium.
The Immune Shield
Beyond mood, Vitamin D is the primary commander of the immune system.
Your white blood cells (macrophages) rely on Vitamin D to produce "cathelicidins"—tiny endogenous antibiotics that tear apart invading bacteria and viruses. There is a reason cold and flu season peaks in January and February. It is not just the cold air; it is the fact that the entire population in the Northern Hemisphere has collectively plummeted into Vitamin D deficiency due to the angle of the winter sun.

Read next: Why Your Vitamin D is Useless Without Magnesium →
The Serotonin Connection: Why Winter Makes You Sad
Here is the mechanism that most doctors overlook. Vitamin D directly regulates the expression of the TPH2 gene, which controls the production of serotonin in the brain. Serotonin is your mood stabiliser, the molecule that antidepressants (SSRIs) are designed to keep elevated. When Vitamin D levels drop below 30 ng/mL, TPH2 expression falls, serotonin synthesis slows, and you begin to experience the hallmark symptoms: low motivation, irritability, social withdrawal, and a pervasive sense of heaviness.
It gets worse. Serotonin is also the precursor to melatonin, your primary sleep hormone. So when Vitamin D drops, serotonin drops, and then melatonin production is compromised. The result is a double hit: you feel low during the day and you cannot sleep properly at night. This is the biochemical engine behind Seasonal Affective Disorder (SAD), and it explains why SAD responds so well to Vitamin D repletion in clinical practice.
The Numbers Are Alarming
If you live above the 37th parallel (which includes the entirety of the UK, Ireland, Scandinavia, Canada, and most of the northern United States), you cannot synthesise any Vitamin D from sunlight between October and March. The sun simply does not reach a high enough angle to deliver UVB radiation to your skin. During these months, you are entirely dependent on supplementation or dietary intake, and the dietary sources (oily fish, egg yolks, fortified milk) provide a fraction of what your body needs.
A 2020 meta-analysis in the British Journal of Psychiatry found that people with Vitamin D levels below 20 ng/mL were 2.3 times more likely to be diagnosed with depression compared to those with levels above 30 ng/mL. This is often considered to be one of the most cost-effective interventions: a blood test costing £30 and a supplement costing £10 per month can resolve symptoms that patients have been suffering with for years.
Clinical Observation
When severely deficient patients begin targeted clinical replenishment (typically high-dose D3 paired with K2 and taken with fat for absorption), blood serum levels reliably normalize within 6 to 12 weeks. Concurrently, patients routinely report a significant lifting of cognitive fatigue and mood stabilization. While cosmetic SPF usage remains important for facial protection, integrating sensible, unprotected sun exposure on the forearms during the summer, paired with winter supplementation, creates a biologically sustainable balance.
An Educational Framework: The 3-Step Solution
We must respect the danger of excessive UV radiation and skin cancer. But we cannot continue to live in total biological darkness. Here is the clinical protocol to restore your master neuro-hormone:
AN EDUCATIONAL FRAMEWORK
1. Test, Don't Guess. Over-the-counter supplementation is useless if you don't know your baseline. Ask your doctor for a 25-OH Vitamin D Blood Test. Your target optimisation zone is between 50 ng/mL and 80 ng/mL.
2. The D3/K2 Synergy. If you are supplementing in the winter, you must take Vitamin D3 (the active form), not D2. Crucially, you must pair it with Vitamin K2 (MK-7). High dose D3 increases calcium absorption; K2 acts as the traffic cop, ensuring that calcium goes into your bones, not your arteries.
View our Clinical-Grade D3/K2 Formula Here →
3. The Magnesium Co-Factor. Your liver and kidneys require heavy amounts of Magnesium as a cofactor to activate the Vitamin D you swallow. If you are magnesium deficient (and 50% of people are), your Vitamin D supplement will remain inactive.
Read our complete guide to Magnesium here →
Clinical Addendum
This information is for educational purposes and does not constitute medical advice. High-dose Vitamin D supplementation can be toxic if not monitored. Always consult your physician and get your blood levels tested before initiating a high-dose replenishment protocol.
If you take one thing from this article, let it be this: test your Vitamin D levels. Ask your GP for a 25-hydroxyvitamin D test. If your level is below 30 ng/mL, you are deficient. Below 50 ng/mL, you are suboptimal. Functional approaches often target 50-70 ng/mL in functional approaches, which typically requires 4,000-5,000 IU of Vitamin D3 daily, taken with a fat-containing meal for absorption. Pair with Vitamin K2 (MK-7, 200mcg) to ensure calcium is directed to bones rather than arteries.